
Acupuncture for Eustachian Tube Dysfunction: Ear Pressure, Popping, and Sinus-Related Blockage
Ear pressure and popping from Eustachian tube dysfunction (ETD) often start upstream, in the nose, sinuses, jaw, and neck, not just in the ear. Acupuncture is a complementary approach that targets ETD symptoms by easing inflammatory congestion, relaxing jaw and neck tension that can interfere with tube opening, and calming the nervous system’s amplification of pressure and discomfort. It works best as part of a combined plan with appropriate medical evaluation and evidence-based ETD self-care. Persistent symptoms, one-sided blockage, or hearing changes deserve formal ear and nasal assessment.
Acupuncture for Eustachian Tube Dysfunction: Ear Pressure, Popping, and Sinus-Related Blockage
Ear pressure and popping from Eustachian tube dysfunction (ETD) often start upstream, in the nose, sinuses, jaw, and neck, not just in the ear. Acupuncture is a complementary approach that targets ETD symptoms by easing inflammatory congestion, relaxing jaw and neck tension that can interfere with tube opening, and calming the nervous system’s amplification of pressure and discomfort. It works best as part of a combined plan with appropriate medical evaluation and evidence-based ETD self-care. Persistent symptoms, one-sided blockage, or hearing changes deserve formal ear and nasal assessment.
Key Takeaways
- ETD is usually an inflammation-and-mechanics problem: nasal swelling plus poor tube opening during swallowing/yawning.
- Acupuncture is most useful when ETD is driven by allergies, sinus congestion, jaw clenching, or stress-sensitive symptoms, not as a stand-alone “cure.”
- Track outcomes with a simple symptom score (like ETDQ-7 style questions) and trigger logging, not just “felt better today.”
- Combine acupuncture with pressure-equalizing techniques, nasal hygiene, and allergy control for the highest payoff.
- Red flags (sudden hearing loss, severe vertigo, fever, drainage, persistent one-sided symptoms) should be evaluated promptly by a clinician.
Why ETD Causes Ear Fullness and Popping (Not Earwax)
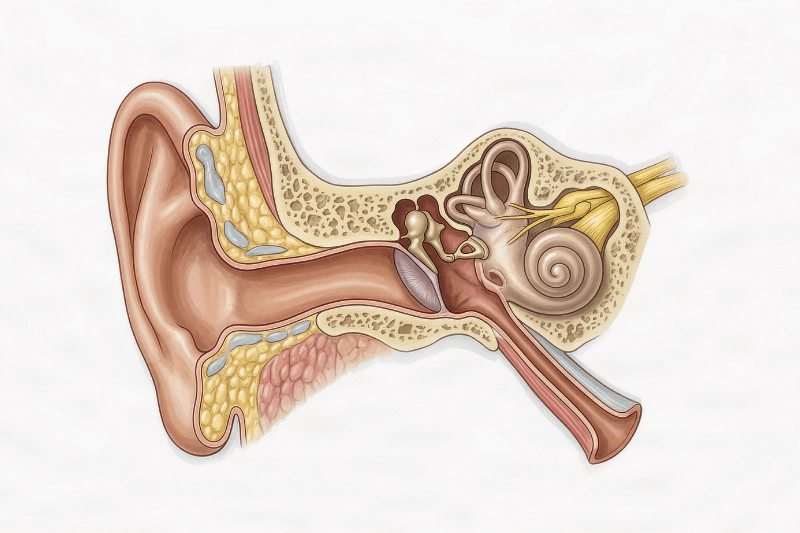
What the Eustachian Tube Does (Pressure Balance + Drainage)
The Eustachian tube is a narrow channel that links the middle ear to the back of the nose and upper throat (the nasopharynx). Its core job is simple: equalize pressure across the eardrum and drain fluid from the middle ear. Most of the time, the tube stays closed. It briefly opens when you swallow, yawn, chew, or change jaw position, letting a small amount of air pass through. That momentary opening is what creates the familiar “pop.”
When the tube does not open reliably, pressure stops equalizing the way it should. The eardrum can feel tight, pulled inward, or slow to rebound, and fluid can linger instead of clearing. This is why ETD often feels like a blocked ear, even though the ear canal itself may be completely clear.
The symptom pattern people describe most often
ETD symptoms usually cluster together rather than showing up as a single complaint. Common descriptions include:
- Ear fullness or pressure (a “plugged” or “underwater” sensation)
- Popping, clicking, or crackling with swallowing or jaw movement
- Muffled hearing or fluctuating clarity
- Discomfort or aching that worsens with colds, allergies, or altitude changes
- Tinnitus and, for some people, light dizziness or imbalance
ETD is also not rare in adults. One U.S. population analysis estimated prevalence around 4.6% using objective middle-ear pressure criteria.
Quick “look-alikes” that mimic ETD (and confuse the diagnosis)
A lot of “ETD” symptoms overlap with other conditions, which is why self-diagnosis can miss the real driver. Here are the most common confounders and the clues that separate them:
- TMJ dysfunction (jaw joint and muscle strain): ear pressure or “popping” that tracks with chewing, clenching, jaw soreness, headaches, or clicking at the jaw hinge.
- Earwax impaction: fullness and muffled hearing that comes from canal blockage, not pressure regulation. Symptoms often do not fluctuate with swallowing or altitude.
- Outer-ear infection (otitis externa): tenderness, itchiness, and pain that increases when the outer ear is touched or pulled, often after swimming.
- Inner-ear or neurologic causes: fullness plus more prominent vertigo, one-sided hearing change, or persistent tinnitus that needs proper evaluation.
This distinction matters for your acupuncture strategy. Inflammation-driven ETD (allergies, sinus congestion) benefits from a different plan than mechanics-driven symptoms (jaw and neck tension), and both differ from conditions that are not ETD at all.
Obstructive vs Patulous ETD
Obstructive ETD (the tube is not opening well)
Obstructive ETD is the more common pattern people mean when they say “my ear won’t pop.” The lining near the Eustachian tube’s opening (in the back of the nose) becomes swollen or congested, often after a cold, during allergy season, or alongside sinus inflammation. That swelling makes it harder for the tube to open properly when you swallow or yawn.
The result is a familiar set of sensations: ear pressure, fullness, muffled hearing, and repeated popping that does not fully relieve the blockage. Symptoms often spike with flying, altitude changes, colds, or nasal congestion, because pressure equalization becomes more difficult when the tube is inflamed.
Patulous ETD (the tube is staying too open)
Patulous ETD is essentially the opposite problem. Instead of failing to open, the tube stays abnormally open more than it should. The hallmark symptom is autophony, which means you hear your own internal sounds unusually loudly, such as:
- your voice echoing in your head
- your breathing sounding “inside your ear”
- sometimes chewing or swallowing sounds amplified
This can feel like pressure or “weird openness,” but it is driven by excess openness, not blockage. Some people experience fluctuating symptoms that can blur the line between patterns, which is why patulous ETD is commonly misunderstood.
Why the type changes the plan
Knowing which pattern you have prevents a “wrong-direction” approach.
- Obstructive ETD: the goal is to reduce inflammation and improve opening mechanics, so pressure equalizes more easily and fluid clears more reliably.
- Patulous ETD: the goal is to stabilize the valve function, and aggressive “decongesting” strategies may worsen symptoms for some people because they can increase dryness and openness.
If autophony is your main complaint (hearing your own breathing or voice loudly in the ear), treat it as a distinct category and get evaluated accordingly, since the treatment strategy is not the same as classic blockage-driven ETD.
The ETD Root-Cause Map: What Usually Drives Ear Pressure and Popping
Nasal and sinus inflammation (allergic rhinitis + chronic rhinosinusitis)
The Eustachian tube opens into the nasopharynx, so anything that inflames the nasal cavity or sinuses can narrow that opening and disrupt normal pressure equalization. This is why ETD commonly flares with seasonal allergies, ongoing nasal congestion, postnasal drip, and sinus pressure. In practice, a “nose-first” pathway is one of the most frequent drivers of persistent ear fullness and popping, especially when symptoms track with pollen seasons, dust exposure, or recurring sinus symptoms.
Post-viral swelling (colds, flu, upper respiratory infections)
ETD often shows up after a cold because mucosal swelling can linger even when the sore throat and cough improve. The tube may open inconsistently for days or weeks, leading to pressure swings, intermittent popping, and muffled hearing that feels unpredictable. If symptoms started right after a viral illness, it is often a sign that inflammation is still present around the tube opening, even if you feel “mostly recovered.”
Jaw and neck mechanics (TMJ, clenching, and tube-opening efficiency)
The tube opens through coordinated muscle action during swallowing and yawning, including the tensor veli palatini. When the jaw, throat, and upper neck are tight, the opening action can become less efficient. This pattern is common in people who clench, grind, or carry chronic neck tension from posture or stress.
ETD is more likely to have a jaw-and-neck component when you also notice:
- jaw soreness or tightness on waking
- headaches or upper neck tightness
- bruxism or daytime clenching
- ear pressure that changes with chewing, yawning, or jaw position
Reflux, irritants, and airway dryness (the “silent inflamer” category)
ENT evaluations sometimes consider inflammatory contributors beyond allergies and infection, including reflux-related irritation (often discussed as laryngopharyngeal reflux) and exposure to irritants such as smoke, vaping aerosols, strong fragrances, or heavy indoor air pollution. Dry air, dehydration, and mouth breathing can also thicken mucus and increase congestion, indirectly making pressure regulation harder.
Pressure-change triggers (flying, diving, mountains)
Altitude and rapid pressure changes stress the Eustachian tube’s ability to open on demand. If the tube is already inflamed or mechanically restricted, flying and diving can make symptoms obvious fast: sharper pressure, repeated popping without relief, or a blocked-ear sensation that lingers after landing.
Structural contributors (when the “plumbing” is crowded)
Sometimes the ssue is not only inflammation but limited space and airflow in the nasal passages. Structurial factors that can keep congestion persistent include turbinate enlargement, deviated septum, or nasal polyps. These do not guarantee ETD, but they can make the upstream nasal environment harder to stabilize, which then keeps ETD symptoms cycling.
Where Acupuncture Fits in ETD Care (And Where It Does Not)
Acupuncture is best used as a complementary therapy for Eustachian tube dysfunction, especially when symptoms are driven by inflammation upstream (nose and sinuses) or mechanics downstream (jaw and neck tension). It is not a substitute for evaluating hearing loss, infection, chronic middle-ear fluid, or persistent one-sided symptoms, which require medical assessment.
Best-fit situations for acupuncture
Acupuncture tends to be most strategic when ETD is linked to one or more of the following drivers:
- Allergic rhinitis or sinus congestion (nasal swelling near the tube opening, postnasal drip, seasonal flares)
- Jaw and neck tension that interferes with normal tube opening during swallowing and yawning (clenching, TMJ overlap, cervical tightness)
- Stress-sensitive symptom amplification, where nervous system arousal makes pressure, fullness, and discomfort feel more intense or persistent
When acupuncture should be adjunctive only
Use acupuncture alongside conventional care, not instead of it, when there is:
- ongoing or recurrent middle-ear fluid (effusion)
- recurrent ear infections or suspected infection
- clear hearing changes, pronounced vertigo, severe ear pain, drainage, or fever
- persistent unilateral symptoms, especially if they are new or worsening
For persistent obstructive ETD with objective findings, ENT care may include targeted nasal disease management and, in selected cases, procedures such as balloon dilation.
What progress realistically looks like (and how to track it)
With ETD, “improvement” is usually functional and trend-based, not instant. Signs you are moving in the right direction include:
- fewer and less intense episodes of fullness or pressure
- popping that becomes easier and more reliable with normal swallowing
- better tolerance for triggers (weather changes, flights, colds)
- reduced jaw and neck tightness that correlates with ear comfort
A practical way to measure progress is a simple daily symptom log plus an ETD symptom score. Many clinicians use the ETDQ-7 (Eustachian Tube Dysfunction Questionnaire-7) framework as a structured way to track symptom change over time.
How Acupuncture May Support ETD
TCM framing: opening pathways and improving fluid movement
In Traditional Chinese Medicine, ear pressure and popping are often discussed through patterns that reflect congestion, inflammation, and constraint in the upper body, such as:
- wind invasion after a cold (acute onset, fluctuating blockage)
- phlegm-damp accumulation (heaviness, mucus, chronic congestion)
- heat in the upper body (irritated nasal passages, inflamed sensation)
- qi stagnation patterns linked to stress (tight jaw, headaches, neck tension)
The clinical goal is not “treating the ear alone,” but supporting drainage, circulation, and functional opening, while addressing the pattern that keeps symptoms recurring.
Biomedical framing: neuromodulation, local tissue effects, autonomic regulation
Modern explanations typically describe acupuncture through mechanisms such as:
- neuromodulation of sensory processing, including discomfort and pressure perception
- local tissue signaling at needled sites that may influence pain and inflammation pathways
- autonomic regulation, which can reduce stress-linked muscle tension and symptom amplification
For ETD specifically, the most practical bridge is indirect and anatomical: acupuncture is often used to reduce nasal-sinus congestion and relieve jaw and neck muscle tension, both of which can affect how reliably the tube opens during swallowing.
The ETD loop that matters most clinically
Many persistent cases follow a repeating three-part loop:
- Nose and sinuses: swelling near the tube opening limits ventilation and drainage
- Jaw and neck mechanics: clenching and cervical tension reduce opening efficiency
- Nervous system gain: symptoms feel louder and more persistent under stress
A well-designed acupuncture plan usually targets mechanics and nervous system tone, while supporting upstream congestion management.
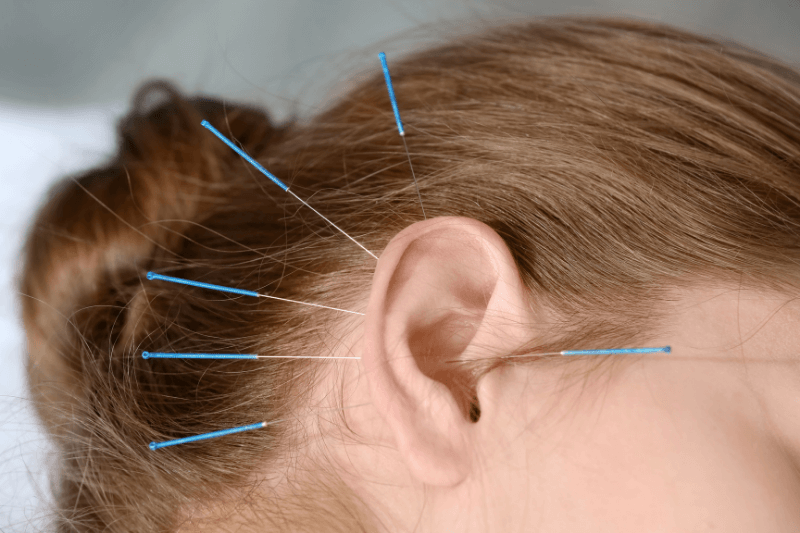
Acupuncture Techniques Commonly Used for ETD
Point selection varies based on whether symptoms look more inflammation-driven, mechanics-driven, or mixed. The examples below reflect common clinical groupings, not a universal prescription. Do not self-needle.
Local ear and jaw region points (pressure, tightness, opening mechanics)
Often used to address perceived fullness and jaw involvement:
- SJ21 (Ermen), SI19 (Tinggong), GB2 (Tinghui)
- SJ17 (Yifeng) for tension patterns around the jaw and ear region
These points are typically used with careful anatomical technique.
Nasal-sinus related points (congestion-driven ETD)
Often considered when ETD tracks with rhinitis, sinus pressure, and postnasal drip:
- LI20, Bitong, Yintang
- LI4 as a common distal support point in face and head patterns
Neck and upper back strategies (swallowing mechanics, cervical contribution)
Used when symptoms correlate with posture strain, clenching, or neck tightness:
- GB20 and upper cervical approaches
- upper trapezius and scalene-related tension patterns, often paired with manual therapy when appropriate
Distal points (systemic inflammation load, fluid patterns, stress load)
Pattern-dependent points often used to support overall regulation:
- ST36 (resilience and systemic regulation)
- ST40 and SP9 (phlegm-damp and fluid pattern support in TCM)
- LV3 for stress-linked tension patterns
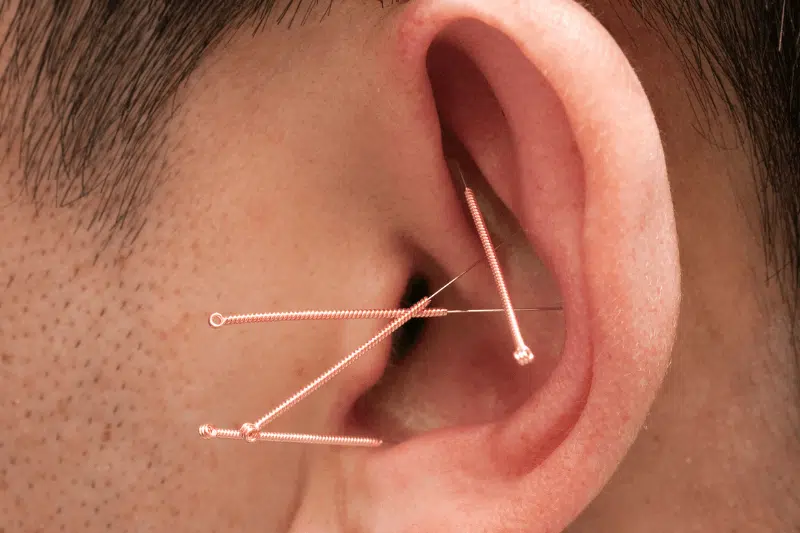
Auricular acupuncture (selected cases)
Auricular acupuncture may be used for autonomic regulation and symptom modulation, but ETD-specific evidence is limited. When included, clinicians generally prioritize techniques that avoid irritation and respect ear anatomy. Safety and sterile technique matter.
What a Treatment Plan Can Look Like
Intake: what a skilled practitioner should clarify
A solid ETD-focused intake typically includes:
- trigger timeline (colds, allergies, flying, diving, weather shifts)
- one-sided vs both-sided symptoms
- autophony screening (to separate patulous patterns)
- jaw clenching, headaches, neck tightness
- symptom scoring (often mapped to ETDQ-7 domains)
Frequency and course of care (typical clinical cadence)
Many plans follow a structure such as:
- 1–2 sessions per week for 2–3 weeks during a flare
- then weekly or biweekly depending on symptom stability
Chronic ETD linked to perennial allergies or chronic sinus inflammation usually needs a longer runway than post-cold ETD.
What people commonly notice during or after sessions
Some people report:
- a more frequent swallowing reflex
- warmth or softening around jaw and upper neck
- transient pressure shifts or popping
- reduced distress or “volume” of the fullness sensation before the mechanics fully normalize
How to measure change in a way that actually reflects function
Track outcomes that correlate with real-life improvement:
- number and intensity of daily pressure spikes
- ability to equalize gently
- hearing clarity and tinnitus intensity trend
- flight tolerance
- jaw and neck tightness on waking
Pair Acupuncture With High-ROI ETD Self-Care (Evidence-Aligned Habits)

Pressure equalization habits (effective when done gently)
Swallowing, yawning, and gentle equalization strategies work because they recruit the tube-opening mechanism. Overly forceful techniques can irritate tissues and worsen discomfort. In ETD, repeatable, gentle strategies generally outperform aggressive “try to pop it harder” attempts.
Nasal hygiene basics (especially for congestion-linked ETD)
When nasal inflammation is driving symptoms, consistency matters:
- saline spray or irrigation (regular, not aggressive)
- humidity support in dry environments
- hydration and reduction of irritant exposure (smoke, heavy fragrance, dry indoor air)
Allergy control and sinus stability (the upstream win)
If your ETD tracks with seasonal flares or daily congestion, stabilizing allergic rhinitis and sinus inflammation is often the difference between short-term relief and long-term recurrence.
Jaw and neck decompression (mechanics support)
These are simple mechanical inputs that can improve opening efficiency in tension-driven patterns:
- keep the jaw “soft” (tongue resting on palate, teeth not touching)
- warm compress at the jaw hinge and upper neck
- slow nasal breathing with longer exhale to reduce tension tone
- brief posture resets (chin tuck + upper back extension)
Conventional Care to Know
What clinicians evaluate in persistent ETD
Common evaluation may include:
- otoscopy (ear exam)
- tympanometry for middle-ear pressure patterns
- hearing testing if symptoms persist
- nasal endoscopy to assess nasal inflammation near the tube opening
Procedures for persistent obstructive ETD
For selected patients with persistent obstructive ETD and objective findings, ENT care may include balloon dilation. Indications and regulatory details can vary by age and device, so this is a clinician-directed decision.
Safety and When to Escalate Care
Typical side effects
Acupuncture is generally low-risk when performed by a qualified practitioner using sterile technique. Common side effects include mild soreness, minor bruising, or transient fatigue.
Use extra caution if you have
- bleeding disorders or anticoagulant use
- immune compromise
- pregnancy (point selection considerations)
- implanted medical devices (relevant for electroacupuncture decisions)
When to see an ENT promptly
Seek medical evaluation urgently or promptly for:
- sudden hearing loss
- severe vertigo or neurologic symptoms
- fever, ear drainage, or escalating ear pain
- persistent unilateral blockage or hearing reduction
Conclusion
Eustachian tube dysfunction is often driven by nasal or sinus inflammation, jaw and neck tension, and pressure-change triggers, not just what is happening inside the ear. Acupuncture can be a helpful complementary therapy for reducing symptom intensity and improving comfort, especially when ETD is linked to allergies, congestion, post-viral swelling, or clenching and TMJ-related tension.
If your symptoms are persistent, one-sided, or paired with hearing changes, severe dizziness, fever, drainage, or worsening pain, seek medical evaluation. For personalized support, contact us to discuss an ETD-focused acupuncture plan tailored to your triggers and root causes.
Sources:
Hamrang-Yousefi, S., Ng, J., & Andaloro, C. (2023, February 13). Eustachian tube dysfunction. StatPearls Publishing.
Shi, F., Ye, Z., Zha, B., Wu, W., Zhang, Y., Yu, L., Liu, W., Rong, Y., & Yang, J. (2025). Recent advances on the mechanism of acupuncture in the treatment of subjective tinnitus. Frontiers in Systems Neuroscience, 19, 1523761
Frequently Asked Questions
Can acupuncture unclog ears from sinus congestion?
Acupuncture is often used as a complementary approach when ETD is driven by nasal or sinus inflammation, especially when paired with consistent sinus hygiene and appropriate medical care for chronic sinus disease.
How many sessions help with ETD pressure and popping?
Many people assess response over 4–8 sessions, tracking symptom frequency and trigger tolerance. Chronic allergy- or sinus-driven ETD often requires a longer plan than post-cold ETD.
Is auricular (ear) acupuncture safe?
Auricular acupuncture is generally safe when performed by a trained professional using sterile technique. The key is anatomical precision and avoiding irritation near the ear canal.
Can ETD go away on its own?
ETD often improves when the upstream driver resolves, such as a cold or short allergy flare. Persistent symptoms or hearing changes should be evaluated to confirm cause and rule out complications.
What is the fastest safe way to relieve ear pressure?
Swallowing and gentle equalization strategies are often first-line because they recruit natural tube-opening mechanics. Avoid repeated forceful attempts if pain increases or symptoms persist.
Is ETD linked to TMJ and jaw clenching?
Yes. Jaw and neck tension can overlap with ETD symptoms, and TMJ dysfunction is a common look-alike. If pressure shifts with jaw movement, a TMJ component is worth assessing.
Contact ACA Acupuncture & Wellness
Get in Touch
Newsletter Sign Up
LOCATIONS
MANHATTAN
QUEENS
NEW JERSEY
CALIFORNIA
ACA Franchise Opportunities
The over $4 billion US acupuncture market offers a great opportunity with over 10% annual growth rates and a continuing flow of new patients interested in the benefits of acupuncture.